Answers Radiology Corner Case #7
Below you will find the answers to Radiology Corner Case #7
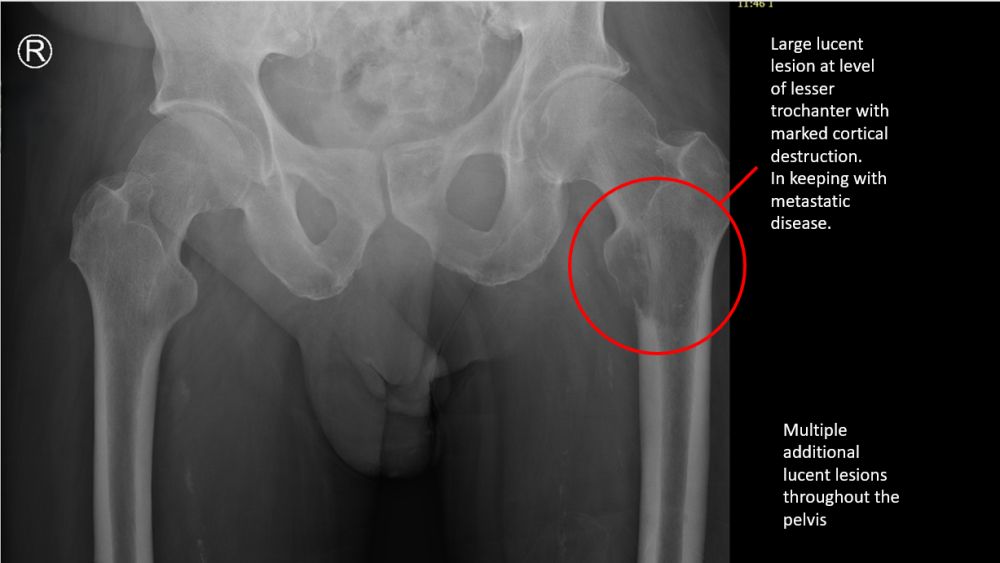
- A 59-year-old man presents complaining of worsening pain in his left leg. He has been experiencing weight loss and lower back pain for some months.
- He has a background history of Oesophageal cancer, Obstructive sleep apnoea, Hypercholesterolaemia, Idiopathic intracranial hypertension.
- He slipped in the shower one week ago and has been able to walk since then, but now the pain is significantly worse and he is unable to do a straight leg raise.
- You arrange an XRay of his pelvis which is shown below. Comment on the X-Rays below.
Click here to get back to Radiology Corner Case #7
What are the treatment options for this condition?
Pathological fractures
- Bone metastases to the long bones will usually lead to pain and pathological fractures.
- If it is first presentation, then a careful history and diagnostic investigations will be required such as:
- CtScan of the chest, abdomen and pelvis- for diagnosis of primary tumour
- PET CT- for dissemination status
- Blood tests for evaluation of general health and fitness for anaesthetic if required
- A bone lesion with an axial cortical involvement of >30mm has a high risk of fracturing and should be managed surgically
- Radiotherapy is the treatment of choice for lesions without risk of fracturing
- The patient in this case had a prophylactic intramedullary nail inserted into his left femur
Click here to get back to Radiology Corner Case #7
A month later………………….
- The patient developed worsening lower back pain, urinary retention and bilateral leg pain.
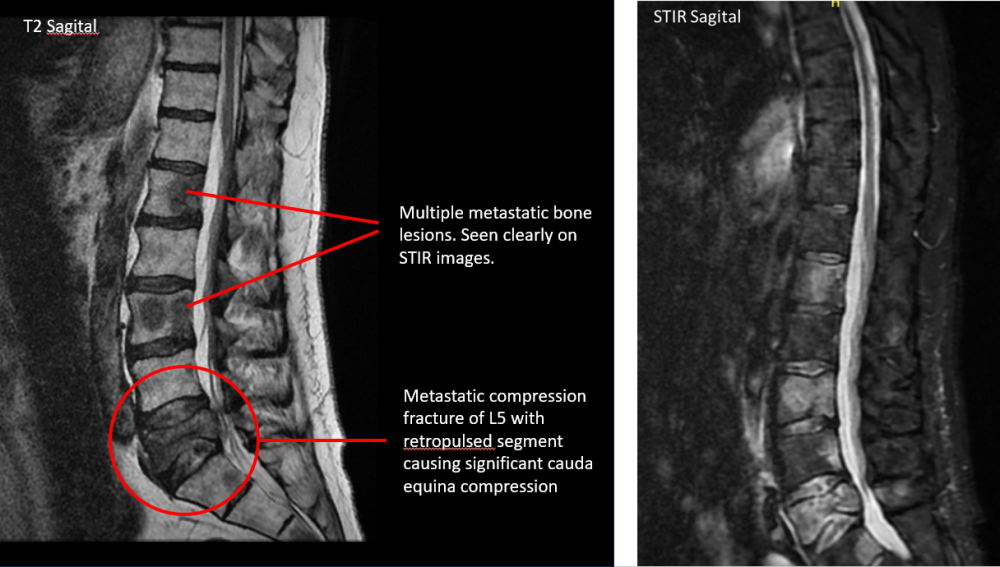
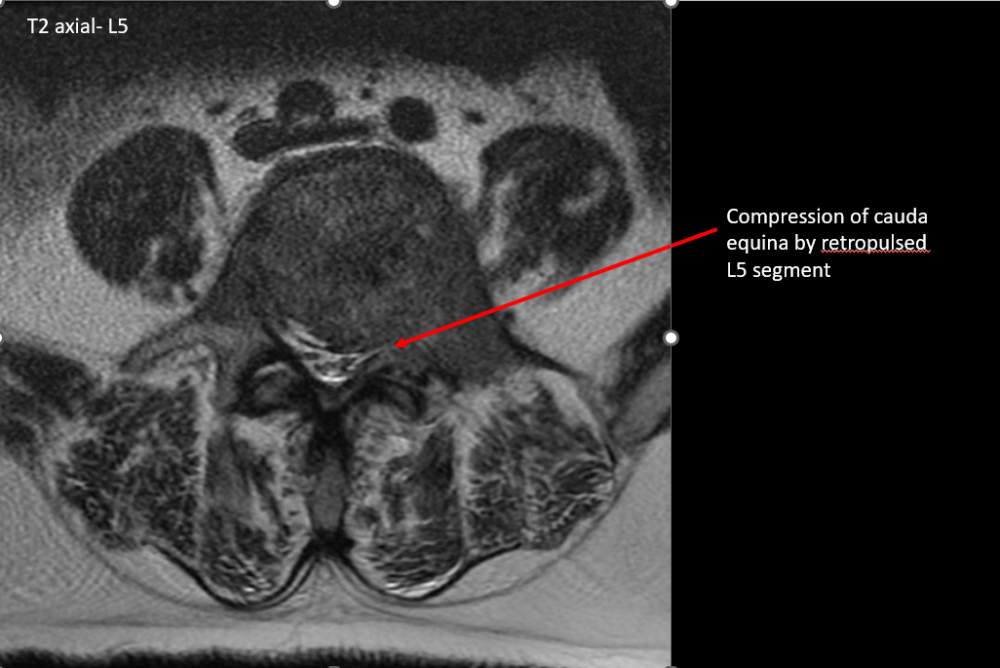
- An urgent MRI scan was arranged to rule out cauda equina syndrome
- Comment on the images
Click to get back to Radiology Corner Case #7
Further points for discussion
What is cauda equina syndrome?
- Cauda equina syndrome refers to a collection of symptoms and signs that result from severe compression of the descending lumbar and sacral nerve roots.
How does this condition typically present?
- It can present acutely or chronically, and it requires two sets of signs:
Perianal and saddle paraesthesia
Bowel, bladder and/or sexual dysfunction
- There are multiple associated symptoms and signs, which may be unilateral or bilateral.
- Lower back pain
- Radiculopathy
- Paraesthesia and/or weakness of lower limbs
- Absent reflexes
Can you think of some common causes?
- There are many conditions which can cause cauda equina syndrome. It is helpful to break them up into categories:
- Degenerative
- Lumbar disc herniation is most common, usually at L4/5 or L5/S1
- Lumbar spinal canal stenosis
- Multiple others e.g. Spondylolisthesis, Haemorrhage into Tarlov cyst, Facet joint cyst
- Inflammatory
- Both acute and chronic form have been seen in patients with longstanding Ankylosing Spondylitis
- Traumatic
- Spinal fracture/dislocation
- Epidural haematoma (may be spontaneous, or post procedural)
- Infective
- Epidural abscess
- Others e.g. Arachnoiditis, Tuberculosis
- Malignancy- Primary or metastatic
- Vascular
- Aortic dissection
- AV malformation
- Degenerative
How is it managed?
- Cauda equina syndrome is generally a surgical emergency
- Surgical decompression within 24 hours has the best outcome
- With metastatic compression, high dose steroids, radiotherapy or intrathecal chemotherapy can also be considered, particularly when surgery is not appropriate due to frailty and other co-morbidities.